
Last updated: March 2026
Syphilis is widely known as a sexually transmitted infection that causes sores and rashes, but most people have no idea it can also steal your vision. This article tells the full story of a real 2022 outbreak in southwest Michigan, centered in Kalamazoo County, in which five women were hospitalized with a rare eye complication of syphilis, all traced back to a single asymptomatic man they had each met online. The case went viral after resurfacing in online communities, and for good reason: it is one of the most alarming documented STI clusters in recent US public health history. This article explains exactly what ocular syphilis is, how to recognize it, why early testing is the only reliable protection, and what the Michigan syphilis cluster reveals about the dangers of untreated syphilis in the modern dating landscape.

People are also reading: STD Testing Best Practices for Polyamorous People
The Michigan Outbreak: What Actually Happened
The cluster began in March 2022, when a woman in southwest Michigan, referred to in the CDC report as Patient A, showed up at a clinic in the Kalamazoo area reporting blurry vision and a fear of going blind. She also had genital lesions. Testing confirmed she had syphilis, and specifically, that the infection had spread to her eyes. Investigators from the Kalamazoo County Health and Community Services Department began tracing her contacts. When they asked her about recent sexual partners, she named a single man she had met through an online platform.
Health officials tried to contact that man. He resisted. He was evasive with investigators, claimed he had left Michigan, and missed a scheduled appointment at a public health clinic. Meanwhile, more women with nearly identical symptoms started appearing. Patient B was hospitalized in April with headaches, hearing loss, worsening blurry vision, and double vision, classic signs that syphilis had reached both her eyes and her nervous system. Patient C tested positive the following month, presenting with a full-body rash, peeling skin on her hands, and spots drifting through her field of vision. Patient D was diagnosed with ocular syphilis by her ophthalmologist in June, along with genital sores and a rash spreading across her hands and abdomen. Patient E reported vision problems in May, and by July, she was admitted to the hospital with both ocular syphilis and neurosyphilis, meaning the infection had reached her brain.
All five women shared the same male sexual partner, each having met him online. Their ages ranged from 40 to 60. None had HIV. None used injection drugs. None engaged in transactional sex. In other words, they didn't fit any of the traditional risk profiles for this type of complication. According to the published case report by Dr. William Nettleton and colleagues, the women had engaged in vaginal sex with the man, and in some cases, oral and anal sex as well. All five were hospitalized and treated with intravenous antibiotic treatment. All recovered. No further cases in Michigan have since been linked to anyone in this cluster.
When public health investigators finally tracked down the common male partner in May 2022, he showed no signs of ocular syphilis, hearing loss, or vision impairment. He appeared symptom-free. But lab tests confirmed he had early latent syphilis, a stage at which the disease has gone quiet internally while remaining fully transmissible. He received treatment. He reported having had multiple female sexual partners during the previous 12 months but declined to identify them. Health officials were left unable to determine how many other people he may have infected before the five documented cases came to light. In parallel, the Michigan Department of Health and Human Services (MDHHS) issued a health advisory through the Michigan Health Alert Network, notifying healthcare providers and surrounding counties about the ocular syphilis cluster and urging clinicians to take thorough sexual histories and test for syphilis in any patient presenting with unexplained eye inflammation.
What Is Ocular Syphilis, And Why Most People Have Never Heard of It
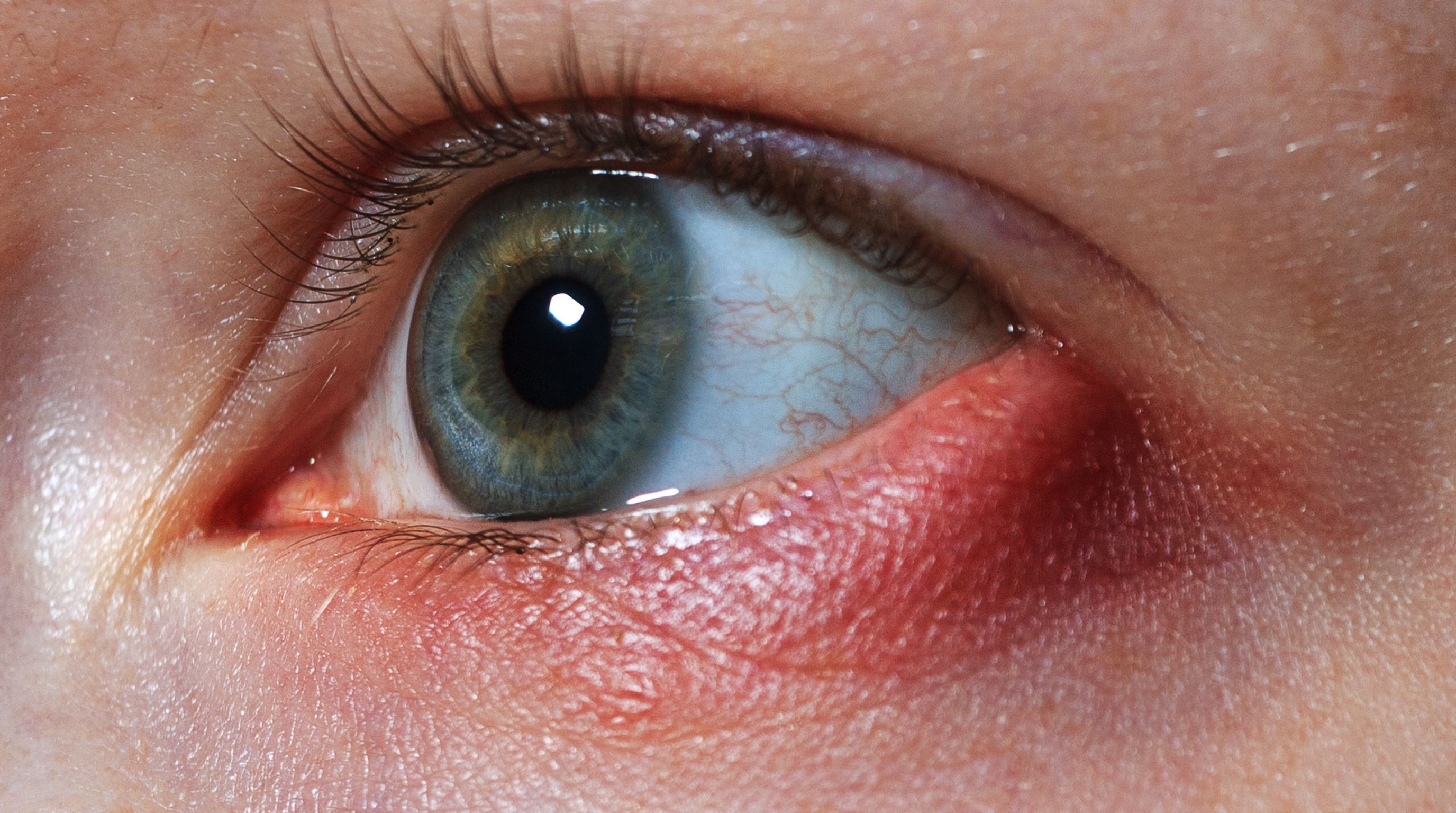
Syphilis is caused by a spiral-shaped bacterium called Treponema pallidum. Most people know it as an STI that causes sores and rashes. What's far less understood is that T. pallidum can travel through the bloodstream and take up residence in virtually any tissue in the body, including the delicate structures of the eye. When that happens, the result is ocular syphilis: an inflammatory infection of the eye that can cause everything from redness and floaters to permanent vision loss and blindness.
The uvea, the layer of tissue beneath the white of the eye, is the most commonly affected structure. Inflammation of the uvea (called uveitis) is the most frequent ocular manifestation of syphilis, and it can be blinding if not treated. But T. pallidum doesn't stop there. It can infect the retina, the optic nerve, the cornea, the conjunctiva, and even the fluid-filled chambers of the eye itself. Each of these locations produces a slightly different set of symptoms, which is one reason ocular syphilis is notoriously difficult to diagnose; it can look like pink eye, uveitis from another cause, a retinal detachment, or a dozen other conditions. Clinicians sometimes call syphilis "the great imitator, " and in the case of the eyes, that nickname is well-earned.
Ocular syphilis was historically associated with late-stage, long-untreated syphilis, the kind that develops over years in someone who never got diagnosed or treated. It was more commonly seen in older patients, people living with HIV, and people who use injection drugs. The Michigan cluster broke every one of those assumptions. These were five women in early-stage syphilis, not late-stage. They were HIV-negative. They were middle-aged, not elderly. And their infections were acquired through heterosexual sex, which had never before been documented as the transmission route in a cluster of this type. According to the CDC's MMWR report, this is the first documented ocular syphilis cluster attributable to heterosexual transmission.
What makes ocular syphilis particularly dangerous is the speed at which it can cause permanent damage. A peer-reviewed study published in the British Journal of Dermatology and available through the National Institutes of Health found that among patients who developed blindness from syphilis, the median time from the onset of eye symptoms to diagnosis was 12 months. That's a year of progressive damage, a gap that researchers attribute to the fact that eye doctors rarely include syphilis in their differential diagnosis when a patient presents with inflammation, making the infection systematically overlooked until serious damage has already occurred..

The Symptoms That Sent Five Women to the Hospital
One of the most dangerous things about ocular syphilis is that its early symptoms are easy to dismiss. Blurry vision, mild floaters, slight eye redness, any of these on their own might send someone to an eye doctor for a routine exam, not to an infectious disease specialist. But when these symptoms appear alongside any recent sexual activity with a new or untested partner, the possibility of syphilis needs to be on the table immediately.
The Michigan women experienced a broad range of symptoms across different eye structures. The table below summarizes the most common presentations of ocular syphilis by affected area:
What made the Michigan cluster unusual, and alarming, is that several of the women presented with more than one of these simultaneously. Patient B had blurry vision and double vision and hearing loss, indicating the infection had moved beyond the eyes into the broader nervous system. Patient E developed full neurosyphilis by the time she was hospitalized in July. The infection hadn't been quietly sitting in one place, it was actively spreading through their bodies, and the eye symptoms were the first visible alarm.
Why Syphilis Without Symptoms Is the Real Danger, And How to Test for It
The man at the center of the Michigan cluster is the clearest possible illustration of why asymptomatic syphilis is such an effective and destructive pathogen. He had no visible sores. He had no vision problems. He had no hearing issues. When investigators finally examined him in May 2022, he appeared perfectly healthy. And yet laboratory testing confirmed he was carrying early latent syphilis, an active infection that he had been transmitting to sexual partners for months without either party knowing it.
Early latent syphilis is what happens after the initial sore heals and the secondary-stage rash fades. The bacteria don't disappear. They retreat into the body and go quiet, the early latent phase is defined as within the first year of infection, during which there are no outward symptoms at all. You can't see it, feel it, or detect it without a blood test. But the infection is still there, still transmissible, and still capable of causing severe internal damage, including, as the Michigan cluster shows, in people you've recently had sex with.
This is the part that doesn't get enough attention in conversations about STI risk: the people most likely to unknowingly spread syphilis are the ones who feel completely fine. They're not hiding an obvious sore. They haven't been feeling sick. They may have had a rash a few months ago that they assumed was a reaction to something, and then it cleared up. In the early latent stage, the body has essentially pushed the infection out of sight, but not out of reach.
The only way to know for certain is to test. And that's where an at-home rapid syphilis test becomes genuinely useful, not as a replacement for regular healthcare, but as a fast, discreet way to get an answer without waiting for a clinic appointment. The Syphilis At-Home STD Test Kit from STD Test Kits detects IgG and IgM antibodies to Treponema pallidum with 99% accuracy, using just a fingertip blood sample. Results are ready in 15 minutes. A negative result means no syphilis antibodies were detected, if taken at the 6-week mark or later, that's reliable reassurance. A positive result means antibodies are present and you need to contact a healthcare provider promptly for confirmation and treatment. There's no lab, no appointment, and no waiting room.
The testing window for syphilis matters more than most people realize. Antibodies become detectable from 6 weeks after exposure, testing any earlier risks a false negative because the immune system hasn't had time to generate a detectable response yet. Test at the 6-week mark for a reliable result. If that result is negative but symptoms develop afterward, retest and seek clinical evaluation immediately. If at any point you develop eye symptoms, skin rashes, or unusual sores, regardless of timing, seek clinical evaluation and tell your doctor to rule out syphilis specifically.
People are also reading: How Soon After Sex Can You Test for STDs?
What the Michigan Cluster Tells Us About Syphilis Strains
One of the most scientifically significant aspects of the Michigan syphilis outbreak is what investigators couldn't explain. The case report was led by Dr. William Nettleton of the Kalamazoo County Health and Community Services Department, working alongside researchers from Western Michigan University Homer Stryker M.D. School of Medicine and the Michigan Department of Health and Human Services, and even with that combined expertise, they couldn't explain why five women, none of whom had HIV, none of whom were in late-stage syphilis, none of whom fit the typical demographic profile, all developed ocular syphilis from the same source. The man himself never developed eye involvement at all. His immune system handled the infection very differently from theirs. Health officials were left with a hypothesis: that the specific strain of Treponema pallidum he carried may have been unusually prone to causing systemic manifestations, particularly in the eyes and nervous system.
This hypothesis couldn't be confirmed. Genetic typing of T. pallidum requires active primary-stage lesions, the open sores present in the earliest phase of infection, from which bacteria can be swabbed and analyzed. By the time Kalamazoo County investigators and MDHHS researchers were able to collect samples, the window for that kind of typing had closed. Only one of the five women had a primary lesion at diagnosis, and the genetic material obtained wasn't sufficient for full strain identification. The man had no lesions at all when examined. So the strain, if it was indeed an unusual one, escaped identification entirely.
What investigators could confirm is this: after all six individuals, the five women and the common male partner, were treated with antibiotic treatment, no further ocular syphilis cases in Michigan were linked back to this cluster. The researchers noted that this pattern suggests the strain may have stopped circulating once the source of transmission was treated. But they were careful to acknowledge that without molecular typing surveillance across a wider geographic area, that conclusion can't be stated with certainty. There could be other people the man infected who were never identified, who may be carrying the same strain today.
The broader scientific implication is uncomfortable: strains of syphilis are not all equivalent. Most syphilis infections do not produce ocular complications. But some strains appear to behave more aggressively, invading tissues that are typically spared. The field of T. pallidum molecular epidemiology is still developing, and the tools needed to identify dangerous strains quickly and routinely in clinical settings don't yet exist at scale. Until they do, the lesson from Michigan is that any syphilis infection, regardless of how mild it appears, carries the theoretical potential for serious systemic complications, and treatment should never be delayed.
The table below breaks down exactly what each patient in the Michigan cluster reported, based on the published CDC case report:
Notice that only one of the women, Patient A, had the classic genital sores typical of primary syphilis at the time of her diagnosis. The others presented primarily with eye and skin symptoms, with the genital signs either absent or already resolved. This is exactly why syphilis gets missed: people, and sometimes their doctors, are looking for sores and don't connect rashes, floaters, or blurry vision to a sexually transmitted infection.
Syphilis Is Still Rising, And the Numbers Should Concern Everyone
The cluster didn't happen in a vacuum. It emerged during one of the most significant syphilis surges the United States has seen in decades. According to CDC data, syphilis cases in Michigan alone climbed from 3.8 per 100, 000 people in 2016 to 9.7 per 100, 000 by 2022, the same year those five Kalamazoo-area women were hospitalized. The Kalamazoo County Health and Community Services Department and the Michigan Department of Health and Human Services had in fact already launched a systemic manifestation surveillance checklist in 2020, specifically to help clinicians in Michigan identify and classify ocular, otic, and neurologic syphilis presentations, a sign that state health officials were already watching the numbers climb and bracing for complications. Nationally, the picture was even starker: reported syphilis cases increased by roughly 80% between 2018 and 2022, rising from approximately 115, 000 to more than 207, 000 cases, the highest numbers recorded since the 1950s.
The most recent CDC surveillance data, released in September 2025 and covering provisional 2024 figures, shows some encouraging signs. Primary and secondary syphilis, the most infectious stages, declined nearly 22% compared to 2023, marking the second consecutive year of decrease. Gonorrhea and chlamydia also fell. Public health officials attributed these declines in part to greater STI awareness and expanded use of at-home rapid tests, which have made testing more accessible to people who might otherwise avoid clinics. The CDC's Division of STD Prevention noted that the combined STI case burden in the U.S. remains more than 2.2 million reported cases annually, 13% higher than a decade ago.
What hasn't improved is congenital syphilis, syphilis passed from a pregnant person to their baby. In 2024, nearly 4, 000 cases of congenital syphilis were reported in the United States, marking the 12th consecutive year of increases and representing a nearly 700% rise from 2015. Babies born with congenital syphilis can experience stillbirth, miscarriage, neonatal death, blindness, deafness, and developmental delays. Every one of those cases is preventable with timely testing and treatment during pregnancy. The fact that the numbers keep rising despite that being true is one of the most troubling data points in modern sexual health.
The Michigan outbreak and these national statistics tell the same story from different angles: syphilis is not a historical disease. It's not something that only affects certain demographics or certain behaviors. It's circulating in communities across the country, spreading silently through people who feel completely healthy, and in rare but documented cases, it is causing catastrophic complications that no one sees coming. The five women in southwest Michigan didn't see it coming either. They went to their doctors for vision problems. Nobody initially thought to test them for an STI.
FAQs
1. Can syphilis really cause blindness?
Yes, and it's more than theoretical. Untreated syphilis can infect the optic nerve, retina, and uvea of the eye. If the optic nerve deteriorates before treatment begins, the vision loss can be permanent and irreversible. The Michigan outbreak involved five women who were hospitalized with vision-threatening eye infections, all from the same syphilis source.
2. How common is ocular syphilis?
It's rare, estimates suggest it occurs in roughly 1% to 5% of syphilis cases involving the nervous system. But "rare" doesn't mean "impossible, " especially as overall syphilis rates remain historically high. The Michigan cluster was unusual even within ocular syphilis cases because it occurred in early-stage heterosexually transmitted infections, not the typical late-stage presentations.
3. What are the first symptoms of ocular syphilis I should watch for?
The most common early signs are blurry vision, floaters (spots or strings drifting across your visual field), eye redness, pain, and sensitivity to light. These are easy to dismiss as minor eye irritation. If you've had unprotected sex with a new or untested partner within the last few months and any of these symptoms appear, get tested for syphilis and see an eye doctor.
4. Can someone spread syphilis without any symptoms?
Absolutely, and this is one of the most important facts about the infection. The man at the center of the Michigan outbreak had early latent syphilis: no sores, no rashes, no visible signs at all. He transmitted syphilis to at least five women and likely never knew he was doing so until public health investigators tracked him down.
5. How long after syphilis exposure should I test?
You should test at 6 weeks after exposure. This is when syphilis antibodies are reliably detectable in your blood. Testing sooner than this will give you a false negative result even if syphilis is present. If you get a negative result at 6 weeks and develop symptoms, get tested again.
6. Can an at-home syphilis test detect early-stage syphilis infection?
Yes. At-home syphilis tests will detect treponemal antibodies in your blood. These are detectable in your blood after the primary infection, once your body has developed an immune response to syphilis. This takes 6 weeks after infection. The STD Test Kits syphilis test is accurate to 99%. While it will not detect syphilis in the very first days after infection, once the standard time period has elapsed, it is very reliable.
7. Is ocular syphilis treatable?
Yes, and the earlier the better. Treatment with intravenous antibiotic treatment can resolve the infection and prevent further damage. All five Michigan women recovered after treatment. However, if the optic nerve is already damaged before treatment begins, the resulting vision loss may be permanent. This is why early detection matters so much, treating syphilis before it reaches the eyes is far simpler than treating it once it's already causing damage there.
8. Could syphilis be misdiagnosed as a regular eye condition?
Very easily, which is part of why ocular syphilis cases often go undetected for months. Syphilitic uveitis looks like uveitis from any other cause. Eye redness from syphilis looks like conjunctivitis. Floaters and retinal inflammation look like a range of other retinal conditions. Doctors who don't ask about sexual history or think to test for syphilis routinely treat the eye symptoms without ever finding the underlying cause.
9. Is syphilis still a major health risk in the US today?
Yes. Despite some recent declines in primary and secondary cases, CDC provisional data from 2024 shows over 2.2 million STI cases annually in the US, with congenital syphilis rising for the 12th consecutive year. Syphilis rates in Michigan specifically more than doubled between 2016 and 2022. The Michigan outbreak is a product of that broader epidemic, not an anomaly.
10. Should I get tested for syphilis if I don't have any symptoms?
If you're sexually active with new or multiple partners, the answer is yes, especially because the most infectious carriers often have no symptoms. Testing when you feel fine is how you catch syphilis before it causes damage. It's also the only way to prevent unknowingly transmitting it to someone else the way the man in the Michigan cluster did for months before he was identified.
Don't Wait for Symptoms, Test Now and Protect Your Vision
The Michigan outbreak is an extreme case, but the lesson it teaches applies to anyone who is sexually active: syphilis is more unpredictable, more dangerous, and more common than most people realize. It doesn't always look like what you expect. It can sit silently in your body for months while you pass it to others. And in rare but documented cases, it can attack your eyes before any other symptom ever appears. The only way to know you don't have it is to test.
The Syphilis At-Home STD Test Kit from STD Test Kits gives you a 99% accurate result in 15 minutes from home, no clinic or prescription needed. If you want broader coverage, because syphilis rarely travels alone, the 7-in-1 Complete At-Home STD Test Kit covers syphilis, HIV, hepatitis B, hepatitis C, HSV-2, chlamydia, and gonorrhea in a single test. One kit, seven answers, at home.
Testing isn't a reaction to something going wrong. It's how you stay in control of your sexual health, and in the case of syphilis, it may be how you protect your eyesight. Visit STD Test Kits to explore the full range of options and find the test that fits your situation.
How We Sourced This: Our article was constructed based on current advice from the most prominent public health and medical organizations, and then molded into simple language based on the situations that people actually experience, such as treatment, reinfection by a partner, no-symptom exposure, and the uncomfortable question of whether it "came back." In the background, our pool of research included more diverse public health advice, clinical advice, and medical references, but the following are the most pertinent and useful for readers who want to verify our claims for themselves.
Sources
5. Ocular Syphilis: Symptoms and Treatment. Cleveland Clinic.
6. Syphilis Eye Infections, While Rare, Are on the Rise. American Academy of Ophthalmology.
About the Author
Dr. F. David, MD is a board-certified infectious disease specialist focused on STI prevention, diagnosis, and treatment. He writes with a direct, sex-positive, stigma-free approach designed to help readers get clear answers without the panic spiral.
Reviewed by: Rapid STD Test Kits Medical Review Team | Last medically reviewed: March 2026
This article is for informational purposes and does not replace medical advice.